Your feet are the starting point for almost everything your body does mechanically. When they are out of alignment, the effects do not stay local. They travel. Knee pain, hip tightness, and chronic lower back ache are frequently traced back to the way feet are hitting the ground, not to any problem in the joints where the pain actually shows up.
This guide covers what foot alignment actually means, the less obvious signs that something is off, what the research says about treatment, and when surgery is the right call versus when it is not.
What Foot Alignment Actually Means
Alignment is about how the bones, joints, and soft tissue of your feet relate to each other under load. When it is correct, body weight spreads across the heel, the lateral arch, and the forefoot in a balanced sequence with each step. When it is not, some parts of the foot absorb far more force than they are built for, and others barely contribute at all.
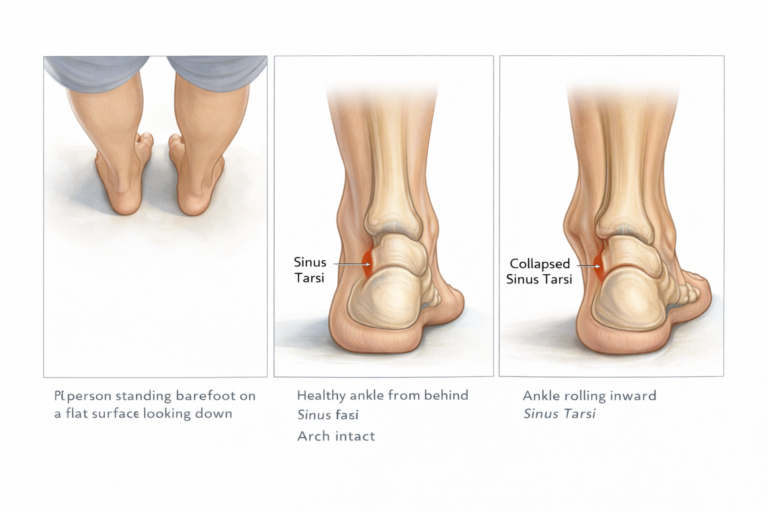
A practical reference point: stand barefoot on a flat surface and look down at your ankles. The ankle bone (talus) should sit cleanly over the front edge of your heel bone (calcaneus), creating a small visible gap between them called the sinus tarsi. When this gap compresses or disappears entirely, the arch has dropped and the foot is no longer transferring load the way it should. Sometimes this is visible from the outside. Often it is not, and imaging is needed to see what is actually happening.
The sinus tarsi collapse is one of the more reliable early markers of developing foot misalignment and one that a podiatrist will look for even when your feet feel fine.
The Three Alignment Patterns
1. Overpronation
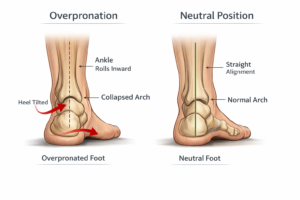
The foot rolls inward past the point where it can efficiently transfer load. The arch flattens under body weight rather than springing back. This is the most common pattern and sits at the root of a long list of problems including plantar fasciitis, shin splints, Achilles tendinopathy, and medial knee stress. Flat feet and overpronation often go together but are not the same. You can have flat feet without notable pain, or significant overpronation with a relatively normal-looking arch.
2. Supination
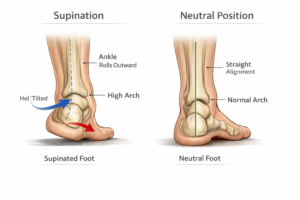
The opposite pattern. The foot rolls outward, loading the outer edge and reducing its capacity to absorb impact. People with high arches tend to supinate. Because the foot stays rigid rather than pronating through its natural range, ground reaction forces hit harder and stress fractures become more likely, especially during high-mileage activity.
2. Neutral
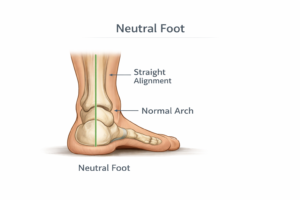
The heel strikes, the foot pronates slightly through the midstance to absorb force, and the toes push off evenly. This is the mechanically efficient pattern. Even a neutral foot can develop alignment problems over time if footwear, injury, weight changes, or age-related tendon weakening shifts the mechanics.
Why Foot Misalignment Causes Pain Elsewhere
The feet are the base of a kinetic chain. When the base is misaligned, every joint up the chain adapts. These adaptations are what create pain in areas that seem unrelated to the feet.
- Knees: Overpronation rotates the tibia inward during each step. This pulls the kneecap laterally out of its groove, creating patellofemoral pain. It also increases compressive stress on the medial compartment of the knee joint, accelerating wear there over time.
- Hips: Asymmetrical foot mechanics create an uneven gait. The hip on the side of greater pronation typically shifts down and inward, placing repetitive strain on the hip flexors, the IT band, and the sacroiliac joint.
- Lower back: Pelvic tilt follows gait mechanics. A foot that rolls in on one side drops that hip slightly with each step, creating a functional leg length discrepancy. Over thousands of daily steps, this asymmetry accumulates as lumbar strain.
- Plantar fascia: Both overpronation and supination overload the plantar fascia, the thick band of tissue along the bottom of the foot. In overpronation it stretches repeatedly beyond its range. In supination it is repeatedly compressed under abnormal load. Plantar fasciitis is one of the most direct downstream results of foot misalignment.
Causes of Foot Misalignment
Most cases have multiple contributing factors layered on top of each other. Genetics determines the starting point. Lifestyle and habits determine how quickly problems develop.
- Structural inheritance: Arch height, joint laxity, and tendon attachment points are largely inherited. People born with flat feet, high arches, or hypermobile joints are starting from a position that requires more support to maintain alignment.
- Footwear: High heels shift the entire body’s center of mass forward. The foot compensates by pronating more aggressively. Worn-out shoes with collapsed midsoles offer almost no arch guidance. Both patterns accelerate misalignment over years of use.
- Previous injury: An ankle sprain that was not fully rehabilitated leaves residual laxity in the ligaments, making future rolling more likely. Stress fractures and tendon injuries change how the foot loads during recovery, often leaving lasting gait alterations.
- Arthritis: Joint surface degradation in the midfoot or ankle disrupts the precise bone positioning that alignment depends on. Rheumatoid arthritis in particular can cause rapid structural change in the feet.
- Posterior tibial tendon dysfunction: This is the single most common cause of adult acquired flat foot. The posterior tibial tendon runs along the inside of the ankle and is the primary active support for the arch. When it weakens or tears, the arch collapses progressively. It is worth naming specifically because it is often missed until the deformity is well advanced.
- Body weight and occupation: Standing on hard surfaces for extended periods under significant body weight accelerates arch fatigue. The structures that hold the arch up are not designed for static load, and they tire under it.
How to Spot Foot Alignment Problems
The symptoms of foot misalignment are often misattributed. People assume their knee pain is from exercise, their back pain is from sitting, and their foot fatigue is just part of a long day. The pattern that should trigger suspicion is pain that is consistently worse after being on your feet and improves with rest, especially if it keeps coming back.
Check your shoes. Uneven wear is one of the most reliable and accessible early indicators:
- Heavy wear on the inner heel and ball of foot = overpronation
- Heavy wear on the outer edge = supination
- Symmetric wear centered on the heel and ball = neutral.
The following table outlines the specific signs to look for and what each one points to:
| Symptom or Sign | What It Points To |
|---|---|
| Ankle rolling inward when standing | Overpronation, collapsed sinus tarsi |
| Shoe wear on inner edge | Flat foot, overpronation |
| Shoe wear on outer edge | High arch, supination |
| Heel or arch pain after standing | Plantar fascia overload |
| Knee pain with no injury | Referred strain from gait misalignment |
| Hip or lower back pain | Compensatory chain reaction upward |
| Bunions or hammertoes developing | Chronic pressure redistribution |
| Foot fatigue within 20 minutes | Inefficient weight transfer through arch |
What Diagnosis Actually Involves
A physical examination is the starting point. A podiatrist will watch you stand, walk, and potentially run, looking at how your ankle tracks over your foot, whether there is collapse at the sinus tarsi, and how your shoes are wearing. They will also palpate the arch, ankle, and the course of the posterior tibial tendon to check for tenderness.
Weight-bearing X-rays are used to assess bone angles under load, which often look quite different from non-weight-bearing films. In cases where tendon damage is suspected, MRI is more appropriate because it shows soft tissue clearly. Gait analysis with pressure-plate technology maps how force is distributed across the foot during walking and provides a precise picture of dynamic mechanics that no static exam can replicate.
Treatment Options
The right treatment depends on what is causing the misalignment, how far it has progressed, and whether the problem is structural or functional.
The table below summarizes when each option applies and what its limitations are.
| Treatment | Best For | What It Does Not Fix |
|---|---|---|
| Custom orthotics | Moderate misalignment, daily pain relief | Underlying bone or tendon structure |
| Targeted exercise program | Flexible flat foot, early-stage misalignment | Rigid structural deformity |
| Supportive footwear | Mild issues, prevention, daily management | Existing arch collapse on its own |
| Corrective surgery | Collapsed sinus tarsi, severe deformity | Gait habits without rehab post-op |
| Physical therapy | Post-injury misalignment, muscle imbalance | Structural bone positioning alone |
Custom Orthotics
Custom orthotics are made from a mold or digital scan of your foot and are designed around your specific pressure distribution and gait pattern. They work by altering where and how force contacts the foot, reducing load on overstressed areas and guiding the foot into better alignment during movement.
The important distinction: orthotics manage the symptoms of misalignment well. They do not fix the underlying structural problem. Someone with a collapsed sinus tarsi wearing orthotics is more comfortable, but the joint is still in the wrong position. This matters because orthotics require consistent use to maintain their effect.
Exercise
The case for exercise as a primary treatment is stronger than most people realize. A randomized controlled trial by Brijwasi and Borkar, published in the Journal of Physiotherapy (2023), put 52 adults with flexible flat foot through either a comprehensive 6-week exercise program or basic ankle range-of-motion exercises. The comprehensive group performed short foot exercises, gluteal strengthening, calf stretching, and dorsiflexion and plantarflexion work three times per week for 30 minutes per session.
After six weeks, the exercise group showed a 0.4 cm greater reduction in navicular drop height and a 16-degree improvement in medial longitudinal arch angle compared to the control group. Both results were precise and statistically meaningful. The authors noted this reduced progression toward more severe flat foot, which is where symptoms typically appear.
The practical implication: for people with flexible flat feet, a structured exercise program targeting not just the feet but the gluteal muscles and calves too, can produce measurable changes in arch architecture. This is not the same as strengthening for general fitness. The exercises need to be specific.
Source: Brijwasi T, Borkar P. A comprehensive exercise program improves foot alignment in people with flexible flat foot: a randomised trial. J Physiother. 2023
Footwear Changes
For mild misalignment, switching footwear is often the single most impactful change someone can make. Motion-control shoes for overpronators, cushioned flexible shoes for high arches, and simply retiring worn-out footwear before the midsole collapses can meaningfully reduce daily strain. Footwear changes work best alongside other treatments, not as a standalone fix for significant misalignment.
Corrective Surgery
Surgery is indicated when conservative treatment has not resolved the problem or when the structural issue is too advanced for non-surgical correction. A common minimally invasive procedure for sinus tarsi collapse inserts a small stent into the sinus tarsi to prevent the ankle bone from shifting inward, restoring the joint relationship without cutting or removing bone. Recovery typically involves a few days of reduced activity rather than weeks of immobilization.
For more complex cases involving tendon damage, significant bone deformity, or joint arthritis, the procedures are more involved, and recovery timelines are longer. A podiatrist can advise on which options are appropriate for the specific diagnosis.
What Happens Without Treatment
Foot misalignment does not stabilize on its own. The structures that are being overloaded gradually weaken, the deformity deepens, and the compensatory patterns in the knees, hips, and back become more entrenched. What starts as occasional arch pain can progress to plantar fasciitis, Achilles tendinopathy, bunion formation, and eventually arthritic change in the ankle and midfoot.
The window where exercise and orthotics can meaningfully reverse or halt the problem is early. Once the posterior tibial tendon tears, or bone positioning shifts significantly, the options narrow toward surgery. This is not meant to alarm, but it is why the persistent mild symptoms that people dismiss for months are worth taking seriously.
Frequently Asked Questions
1. Can foot alignment problems cause knee or back pain?
Yes. Overpronation rotates the tibia inward and creates knee tracking problems. The same gait asymmetry alters pelvic position, contributing to lower back pain.
2. Is flat foot the same as foot misalignment?
Not always. Flat feet describe arch shape. Misalignment describes how the bones and joints are positioned. You can have flat feet without significant misalignment, or develop misalignment over time as flat feet worsen under load.
3. Are custom orthotics better than store insoles?
Custom orthotics are built around your specific foot mechanics, not a generic arch profile. For moderate to significant misalignment, they are considerably more effective than prefabricated insoles.
4. Can the right exercises actually change the shape of my arch?
For flexible flat feet, yes. Clinical research shows a structured 6-week program can measurably improve navicular drop height and arch angle. This does not apply to rigid structural deformities.
5. When should I see a podiatrist?
If foot, knee, hip, or lower back pain persists for more than a few weeks, recurs after activity, or is getting progressively worse, a podiatrist evaluation is the right step. Earlier assessment means more treatment options.
6. Is surgery painful or risky?
Minimally invasive procedures like sinus tarsi stenting have short recovery periods and low complication rates. More complex surgeries carry higher risk and longer recovery and are reserved for severe cases.
7. Can children have alignment problems?
Flexible flat feet are common and often self-correct before adolescence. Persistent pain or flat feet that do not improve by around age 8 to 10 warrant a podiatric assessment.
8. Does foot misalignment get worse with age?
Yes, gradually. Tendons lose elasticity, stabilizing muscles weaken, and years of suboptimal loading accumulate. This is why people who manage mild flat feet without issues for decades sometimes develop pain in their 40s and 50s.