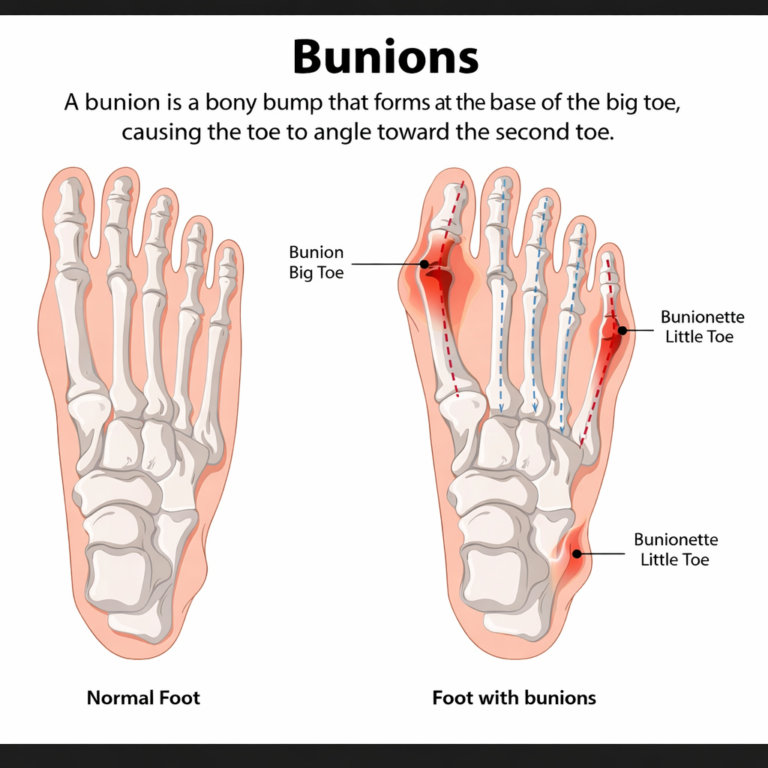
A bunion is a bony bump that forms at the base of the big toe. It develops slowly, usually over years, and in many cases people do not notice it until there is pain or difficulty wearing shoes. Bunions are more common than most people realise. Research suggests they affect roughly one in three adults, with women being affected more often than men due to footwear patterns and anatomical differences. Surgery is often mentioned as the only solution, but that is not accurate. A review published in the Indian Journal of Integrative Medicine concluded that non-surgical treatments for bunions deserve greater clinical attention, noting that surgery does not always fully restore normal function and long-term pain frequently follows surgical intervention. Non-surgical management is not just a stopgap. For many people, it is the main treatment plan.
This guide explains what bunions are, what causes them, how to identify different types, and what non-surgical options are available to manage them.
What Is a Bunion
A bunion, medically known as hallux valgus, is a structural deformity of the foot. The term “hallux” means big toe, and “valgus” refers to the toe angling outward toward the other toes. As this angle develops, the first metatarsophalangeal (MTP) joint, where the big toe connects to the foot, is pushed out of alignment. Over time, the joint protrudes outward, forming the visible bump associated with bunions.
The bump itself is not a growth of new bone. It is the displaced joint. The skin over it can become red, swollen, or calloused from constant friction inside a shoe.
According to Cleveland Clinic, bunions form when pressure is applied to the big toe joint for a long period of time, gradually pushing it out of its natural position. The process is slow and often painless in early stages, which is why many people do not act until the condition has progressed.
What Causes Bunions
There is no single cause. Bunions develop from a combination of factors, including inherited foot structure, footwear choices, and certain medical conditions. Any one of these alone may not be sufficient, but together they create the conditions for a bunion to form.
| Cause | How It Contributes |
|---|---|
| Inherited foot mechanics | More than 70% of people with bunions have a biological parent who had them. The way bones and joints are shaped is largely genetic. |
| Narrow or pointed footwear | Shoes with a tight or pointed toe box force the toes into an unnatural position. Over years of daily use, this can shift the MTP joint out of alignment. |
| Flat feet and overpronation | When the arch collapses inward during walking, the big toe bears more rotational force, accelerating joint deviation. |
| Inflammatory conditions | Rheumatoid arthritis and lupus cause inflammation in joints, including those in the foot, which can change bone structure over time. |
| Occupation | Jobs that require prolonged standing, including nursing, teaching, and retail, increase the cumulative pressure on the forefoot. |
| Abnormal foot mechanics | The way a person walks, distributes weight, or compensates for other issues can place uneven stress on the big toe joint. |
Key point
Bunions do not reverse on their own. Once the joint has shifted, it will not return to its natural position without intervention. The goal of non-surgical care is to slow progression and manage symptoms, not to reverse the deformity.
Who Is at Risk
Certain groups are more likely to develop bunions:
- Women are affected at higher rates than men, largely due to footwear patterns involving narrow toe boxes and heels, along with differences in joint laxity.
- People with a family history of bunions are significantly more likely to develop them. The structural predisposition is inherited.
- People with flat feet are at higher risk because the inward rolling of the foot creates abnormal loading on the big toe joint.
- Older adults face increased risk as tendons, ligaments, and joint capsules weaken with age.
- Athletes and active individuals who train heavily, particularly those in sports involving repetitive pivoting or lateral movement.
- People with rheumatoid arthritis or similar inflammatory joint conditions.
Symptoms of a Bunion
The most obvious sign is the visible bony bump on the inner edge of the foot at the base of the big toe. Beyond that, symptoms vary depending on how far the deformity has progressed.
| Symptom | What It Means |
|---|---|
| Bony bump at the base of the big toe | The displaced MTP joint. Usually the first visible sign. |
| Pain or aching around the joint | Can be constant or come and go with activity or footwear. |
| Redness and swelling over the bump | Caused by friction and inflammation inside the shoe. |
| Difficulty bending or moving the big toe | A sign of joint stiffness, which typically worsens as the deformity progresses. |
| Corns or calluses | Thickened skin that forms where the toes rub against each other or against the shoe. |
| Hammertoes forming on the second toe | The displaced big toe pushes the second toe upward, causing it to bend abnormally. |
| Numbness near the big toe | Nerve compression from the bulging joint or from tight footwear. |
| Pain worsening with shoes on | The bump presses directly against shoe material, especially narrow or hard-sided footwear. |
Symptoms are not always present in early stages. A bunion can be visually obvious before it causes any pain. This is important because it means treatment started early, before pain appears, has the best chance of limiting progression.
Types of Bunions
Not all bunions are the same. The type affects where the deformity appears, why it developed, and what treatment approach is most appropriate.
| Type | Description | Who It Affects |
|---|---|---|
| Hallux Valgus (Standard Bunion) | The most common type. A bony bump on the inner edge of the foot at the base of the big toe, caused by the MTP joint being pushed out of alignment. | Adults, most commonly women; often linked to footwear and inherited structure |
| Tailor's Bunion (Bunionette) | Forms on the outer edge of the foot at the base of the little (pinky) toe. Less common but causes similar friction, pain, and swelling. | People who wear narrow shoes; those with splayed forefoot |
| Congenital Bunion | Present from birth. The foot is structurally deformed before weight-bearing begins. Relatively rare. | Newborns; diagnosed in infancy |
| Juvenile or Adolescent Hallux Valgus | Develops before the age of 18, often in children and teenagers with a strong family history. Treatment approach differs because the foot is still growing. | Children and teenagers under 18 |
| Acquired Bunion (Secondary to Arthritis) | Develops as a result of inflammatory joint disease such as rheumatoid arthritis, which destroys joint cartilage and changes bone alignment. | People with rheumatoid arthritis or other inflammatory conditions |
Bunion Severity: A Simple Classification
Clinicians often assess bunion severity using the angle between the first metatarsal and the big toe. This angle, called the hallux valgus angle (HVA), is measured on an X-ray. The broader the angle, the more severe the deformity.
| Stage | Hallux Valgus Angle | Typical Presentation |
|---|---|---|
| Mild | Less than 20 degrees | Small bump visible; little or no pain; most shoes still fit |
| Moderate | 20 to 40 degrees | Visible bump with swelling; pain with activity or tight shoes; second toe may begin to overlap |
| Severe | Greater than 40 degrees | Significant deformity; constant or near-constant pain; difficulty finding suitable footwear; hammertoe development common |
Mild and moderate bunions respond well to non-surgical management. Severe bunions with substantial functional limitation are more likely to require surgical evaluation, though non-surgical measures still play a role in post-operative recovery.
Complications If Left Untreated
Bunions are progressive. Without any management, the deformity typically worsens over time. The rate of progression varies by individual, but the direction is consistent. Complications that can develop include:
- Hammertoes: The misaligned big toe pushes the second toe upward, forcing it into a permanently bent position.
- Bursitis: The fluid-filled sacs that cushion the joint can become chronically inflamed, adding to pain and swelling.
- Osteoarthritis: Long-term abnormal joint mechanics accelerate cartilage wear in the MTP joint, leading to degenerative arthritis.
- Corns and calluses: Persistent friction causes thickened skin that can become painful and prone to breakdown, particularly in people with diabetes.
- Altered gait: Pain avoidance changes how people walk. These compensation patterns create downstream problems in the knees, hips, and lower back.
- Metatarsalgia: Ball-of-foot pain develops when weight shifts away from the painful big toe during walking.
Non-Surgical Treatment Options
Non-surgical treatment is the first line of management for bunions at every severity level. The aim is to reduce pain, slow progression, and maintain function. According to HealthPartners, most people do not need surgery to manage their bunion symptoms, and non-surgical approaches are always the first step regardless of severity.
1. Footwear Modification
The most impactful change most people can make immediately. Shoes with a wide toe box reduce pressure on the MTP joint and stop the big toe from being pushed inward. The shoe should not pinch the toes together at any point. Heels above 2.5 cm increase forefoot loading and should be avoided or minimised. Soft, flexible uppers reduce friction over the bunion. Trying shoes on later in the day is advisable since feet are slightly larger by evening.
Key features to look for in footwear:
- Wide, rounded toe box with adequate depth
- Firm but cushioned sole
- Low or no heel
2. Bunion Pads and Cushioning
Gel or moleskin pads placed over the bunion create a buffer between the bony prominence and the shoe. They do not correct the deformity but reduce the direct friction and pressure that cause day-to-day pain. These are particularly useful for people who need to wear formal or uniform footwear.
3. Toe Spacers
A soft spacer placed between the big toe and second toe pushes the big toe back toward a more neutral position. It cannot permanently realign the joint, but it reduces the angle under which the toe is held during rest or light activity, which can provide meaningful pain relief over time. Toe spacers are generally worn inside shoes.
4. Night Splints
A bunion splint is worn while sleeping and holds the big toe in a straighter position. It cannot reverse the structural deformity, but consistent use can reduce morning stiffness and help slow the rate at which the angle worsens. Splints are not compatible with most footwear and are intended for overnight use only.
5. Pain Relief Medication
Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen reduce both pain and swelling. They are appropriate for acute flare-ups but are not a long-term solution. They should not be taken for more than 10 consecutive days without medical guidance. Topical NSAID creams are an alternative for those who prefer not to take oral medication.
6. Cold and Heat Therapy
Applying ice or a cold pack wrapped in a thin cloth for 15 to 20 minutes reduces acute swelling and provides temporary pain relief. Warm water soaks can help with stiffness and general soreness in the joint. Elevating the foot while icing amplifies the anti-swelling effect.
7. Physical Therapy
A physiotherapist can assess gait mechanics, identify compensatory patterns, and prescribe specific exercises to strengthen the muscles around the big toe and arch. Maintaining or improving the range of motion in the MTP joint slows the development of joint stiffness and reduces overall pain. Ultrasound therapy and massage are also used in clinical physiotherapy for bunion management.
8. Weight Management
Excess body weight increases the load on the forefoot with every step. Even a modest reduction in body weight reduces the cumulative force passing through the MTP joint over thousands of daily steps, which can meaningfully slow bunion progression.
How Insoles and Orthotics Help
Custom orthotics are one of the most effective non-surgical tools for managing bunions. Their role is not to push the bunion back into place but to address the underlying mechanics that are driving the deformity forward.
When the arch collapses inward (overpronation), it pulls the big toe outward with each step, progressively worsening the hallux valgus angle. A well-made orthotic supports the arch, reducing the inward rotation that loads the MTP joint asymmetrically. Over time, this reduces both pain and the rate at which the deformity advances.
According to Cleveland Clinic, both over-the-counter and custom-made orthotic inserts are part of standard bunion treatment protocols. Custom orthotics are more precisely shaped to an individual’s foot and gait and are generally more effective for moderate and severe cases or for people with coexisting foot conditions like flat feet or plantar fasciitis.
For bunion management, orthotics are typically designed to:
| Orthotic Feature | Effect on Bunion |
|---|---|
| Medial arch support | Reduces inward rolling; limits the rotational force on the MTP joint with each step |
| Deep heel cup | Stabilises the rearfoot to prevent the chain of movement that drives pronation forward |
| Metatarsal pad | Redistributes forefoot pressure away from the big toe joint, reducing pain during walking |
| Toe alignment element | Some custom designs include a toe post or spacer built into the insole to maintain a more neutral big toe position |
| Wider forefoot base | Allows the toes to spread naturally rather than being compressed toward the midline |
For Indian footwear contexts
Many Indian footwear styles, including formal shoes, sandals, and sports shoes, do not come with adequate arch support. If you wear footwear for long periods, particularly on hard floors or concrete, adding a custom insole significantly reduces the cumulative load on the forefoot.
Exercises for Bunion Management
Strengthening the muscles around the big toe and arch can slow the progression of a bunion and reduce pain. The exercises below are generally safe to start at home but check with a physiotherapist if you have moderate to severe symptoms before beginning.
| Exercise | How to Do It | Target |
|---|---|---|
| Toe Curls | Sit with feet flat on the floor. Curl and spread toes repeatedly for 10 to 15 reps. | Intrinsic foot muscles; improves toe control |
| Marble Pickups | Use your toes to pick up small objects from the floor and place them in a container. | Forefoot dexterity and muscle strength |
| Big Toe Stretch | Gently pull the big toe back toward a neutral position using your hand. Hold for 10 to 30 seconds. | MTP joint mobility; soft tissue flexibility |
| Towel Scrunches | Place a small towel on a smooth floor. Use your toes to scrunch it toward you. | Arch and toe flexor strength |
| Calf Raises | Stand on the edge of a step with heels hanging off. Rise onto your toes slowly, then lower. | Calf and posterior tibial tendon strength; reduces arch collapse during walking |
| Arch Doming | Sit with feet flat. Without curling toes, try to shorten and lift the arch of your foot without raising your toes. Hold 5 seconds, repeat 10 times. | Deep intrinsic arch muscles; primary support for the medial arch |
When Surgery Becomes Necessary
Surgery is not the first step. It is considered when non-surgical management has been tried consistently and has not provided adequate relief, or when the deformity has progressed to a degree that it significantly limits daily function.
Signs that a surgical evaluation may be appropriate:
- Persistent pain that does not respond to footwear changes, orthotics, and physiotherapy after several months
- Inability to walk comfortably for normal daily activities
- Progressive deformity despite conservative management
- Development of significant secondary complications such as severe hammertoe or joint arthritis
People who undergo bunion surgery are typically able to resume all normal activities within two to three months. However, the post-operative period requires orthotics and careful footwear management to prevent recurrence. Surgery corrects the structural deformity but does not address the mechanical patterns that caused it. Without continued support, bunions can recur after surgery.
The Indian Journal of Integrative Medicine review specifically noted that surgery is not adequately restoring full patient outcomes in all cases, and that non-surgical approaches should be explored more thoroughly before committing to surgical intervention.
Prevention and Slowing Progression
If you have a family history of bunions or an inherited foot structure that predisposes you to them, prevention means delaying or limiting progression rather than eliminating the possibility entirely. The practical steps overlap with treatment:
- Wear shoes with adequate toe room and low heels consistently, not just when you notice pain.
- Have your foot mechanics assessed if you have flat feet or a history of overpronation. A custom insole can reduce the rotational force on the MTP joint before a bunion begins to form.
- Avoid prolonged periods in narrow or pointed footwear, particularly high heels with a narrow toe box.
- Keep the muscles of the foot and calf strong through regular exercise.
- If you notice a small bump beginning to form, act early. The earlier the intervention, the easier it is to slow progression.
Frequently Asked Questions
1. Can a bunion go away on its own?
No. Once the joint has shifted, the deformity is permanent unless corrected surgically. Non-surgical treatment manages pain and slows progression but does not reverse the structural change.
2. Are bunions only caused by shoes?
No. Footwear is a contributing factor but not the only cause. Inherited foot structure and gait mechanics are often the primary drivers. Shoes accelerate an already present predisposition. Many people who wear sensible shoes still develop bunions due to genetic structural factors.
3. Can insoles fix a bunion?
Insoles cannot reverse the deformity or push the joint back into place. What they can do is correct the underlying foot mechanics, particularly overpronation, that are contributing to the deformity’s progression. This reduces pain and slows the rate at which the bunion worsens.
4. Do bunions affect both feet?
Yes, in many cases. Bunions often develop on both feet, though one side may be more advanced than the other. Bilateral bunions are common in people with inherited structural predispositions.
5. Can children get bunions?
Yes. Juvenile hallux valgus affects teenagers and occasionally younger children, usually in families with a strong genetic history. Treatment for adolescents differs from adults because the foot is still growing, and surgical correction is generally deferred until skeletal maturity.
6. When should I see a podiatrist?
See a podiatrist if you notice a visible bump at the base of your big toe, have persistent pain when walking or wearing shoes, notice your big toe beginning to angle toward the second toe, or if you are having trouble finding shoes that fit comfortably. Early assessment leads to better outcomes.
7. Does bunion severity affect treatment?
Yes. Mild bunions respond well to footwear changes, pads, and orthotics alone. Moderate bunions may also benefit from physiotherapy and toe spacers. Severe bunions with constant pain and significant functional limitation are more likely to be considered for surgical evaluation, though non-surgical measures are still part of overall management.
8. Can bunions come back after surgery?
Yes. Recurrence is possible if the underlying mechanical causes are not addressed. Wearing appropriate footwear, continuing to use orthotics, and maintaining foot strength are important post-surgical habits that reduce the likelihood of recurrence.